About the Authors
New research and technological advances continue to pave the way for more predictable results with implant therapy. Today, patients demand esthetic replacements for their missing teeth with shorter treatment times and minimal downtime or inconvenience. To this end, the immediate loading of dental implants in a predictable and organized manner has been a long-sought-after goal. The emergence of computed tomography (CT) planning software, coupled with the fabrication of accurate implant surgical guides and precise surgical instrumentation, has provided clinicians with the ability to plan and implement the placement of implants without raising a flap, along with an esthetic provisional restoration in one short visit. 1-3 Patients can leave the office with tooth-colored, esthetic, fixed provisional restorations, thus providing a great psychological benefit and a high level of patient satisfaction.
A 58-year-old man presented with failing dentition in the maxillary arch. The diagnosis included inadequate bone quality and quantity for implant placement without the need for grafting/socket preservation but adequate interocclusal clearance with the opposing natural dentition. The patient desired a fixed restoration. The consultation included a treatment plan for placement of implants with CT-guided implant surgery and immediate provisionalization with a fixed restoration on the same day as implant placement. The treatment plan included:
Case Presentation
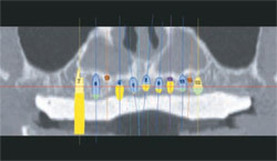
PRESURGICAL TREATMENTThe remaining hopeless teeth were ex-tracted, socket preservation was performed to preserve the ridge width and height (Figure 1), and an immediate denture was placed. The complete denture, which was satisfactory with regards to fit, esthetics, and phonetics, was duplicated in a mixture of 30% barium sulfate and cold-cure acrylic resin (Figure 2). The duplicate denture/scanning appliance was to be worn during the exposure of the patient’s CT scan. The appliance provided a surgical guide for dental implant surgical planning in relation to tooth position, as well as outlining the soft tissues of the edentulous maxilla so that a tissue-supported surgical guide could be fabricated. The scanning appliance was placed intraorally, equilibrated, and a Blu-Mousse (Parkell, Inc, Edgewood, NY) bite registration was made. This bite registration would allow the master cast, which would be poured into the surgical guide, to be articulated against the lower cast, using the scanning appliance. The surgical plan was developed on SimPlant Planner Interactive CT Planning Software, version 10.4 (Materialise Dental, Inc). Angulated abutments were planned on the four most posterior implants. This was possible because the Navigator™ System For CT Guided Surgery (BIOMET 3i) incorporates positioning grooves on the master tubes which are placed in the surgical guide, allowing the rotation of the implant hex to be the same in the patient as the rotation of the analog hex on the master cast. A CT scan was obtained with 1-mm axial sections and the occlusal plane at a 0° gantry angle, following the Materialise radiographic protocol. The DICOM data was then processed using SimPlant Pro Software. To evaluate the surgical bone volume and anatomic structures, virtual implants were placed into the reformatted images. Virtual angulated abutments were also placed on the implants where indicated to ensure emergence of the screw access hole in the proper location. The relationship of the planned implant/abutment positions to the bone of the edentulous ridge can be seen in Figure 3. The surgical plan was saved and sent to Materialise via the Internet for fabrication of the surgical guide. The surgical guide incorporates master tubes designed specifically for the Navigator System (Figure 4), which provides for implant placement in four dimensions (buccal/lingual, mesial/distal, occlusal/apical, and rotation of the hex).
To fabricate a provisional restoration for immediate placement at the time of implant placement, appropriate diameter and length implant analog mounts were selected from the Navigator Laboratory Kit (BIOMET 3i). The implant analog mounts were mated with the appropriate analog and inserted into the master tube (Figure 5). Great care was taken to ensure that the rotational positioning grooves on the master tubes were engaged with the pin on the analog mounts to establish the proper alignment of the analog and implant hexes from the cast to the mouth. When full seating was verified, the thumb screws on the mounts were tightened to lock each assembly into the master tubes. The guide was then beaded and boxed and a soft tissue master cast was poured (Figure 6). The thumb screws were loosened, the analog mounts were removed from the guide, and the guide was removed from the master cast. The scanning appliance was then placed on the master cast and articulated with the lower cast using the previously obtained bite registration (Figure 7). The appropriate-sized Conical Abutments (BIOMET 3i), were then placed on the analogs in the cast. During the planning of the case, two of the implants were selected to employ screw retention and the remaining implants were designed to employ QuickBridge Provisional Components as retentive elements. The decision as to which implants to screw retain was based on a bone density analysis performed around each implant as measured in Hounsfield units in the SimPlant Planner software. The QuickBridge Titanium Cylinders were placed onto the Conical Abutments and tightened (Figure 8). QuickBridge Caps were snapped onto the QuickBridge Titanium Cylinders. Undercuts in the caps were waxed out, and the cast was then duplicated and articulated (Figure 9). The provisional restoration was then waxed on the duplicate cast, invested, and processed. After processing, one Conical Temporary Cylinder was incorporated into the provisional restoration in the laboratory using cold-cure acrylic resin (Figure 10). The second Conical Temporary Cylinder was incorporated into the provisional restoration intraorally after implant placement and before the pick-up of the QuickBridge Caps. This was done to compensate for any scanning error and to ensure a completely passive fit of the provisional restoration.
SURGICAL TREATMENTThe patient was anesthetized using 2% xylocaine with 1:100,000 epinephrine. The surgical guide was placed intraorally. Soft tissue punches, drill positioning handles, and twist drills with drill stops were selected from the Navigator Surgical Kit (BIOMET 3i) using the surgical plan received from Materialise. The rotary tissue punches were passed through the guide tubes while the guide was held in position manually. The tissue punch was rotated with the implant drilling unit set at a low speed until the bone crest was felt. The guide was removed from the mouth and the tissue cores were removed with hand instruments. The guide was then replaced and fixated using 2-mm diameter bone screws (BIOMET Microfixation, Jacksonville, FL) (Figure 11). The surgery began with the use of a cortical punch/countersink drill to shape the bone crest and pilot the osteotomies. The osteotomies were prepared through the master tubes using the appropriate drill positioning handles and twist drills with drill stops. The proper diameter and length implant mounts were selected from the kit and placed into the internal interface of the implants. The implants were threaded into place through the master tubes using the drilling unit on slow speed. Final seating of each implant was accomplished using a hand ratchet to ensure that the positioning groove on the implant mount matched the rotational positioning grooves on the master tube for each location (Figure 12). Each implant mount was loosened and removed, followed by the removal of the bone screws and the surgical guide. Manual bone profilers were then used to profile the bone coronal to the implant prosthetic seating surface.
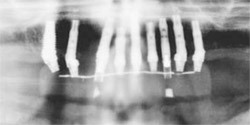
IMPLANT PROVISIONALIZATIONConical Abutments were then placed and secured with abutment screws tightened to 20 Ncm of torque. QuickBridge Titanium Cylinders were placed onto each abutment and hand tightened. The remaining Conical Temporary Cylinder was then placed and secured with a retaining screw (Figure 13). The provisional restoration was placed and equilibrated, and the remaining Conical Temporary Cylinder was luted with cold-cure acrylic resin. A lubricated cotton tip applicator was placed to prevent acrylic from flowing into the screw access opening (Figure 14). The wooden tip was removed and the patient was brought into centric occlusion before complete setting of the acrylic resin. After the acrylic resin had set, the provisional restoration was removed. QuickBridge Caps were snapped onto the QuickBridge Titanium Cylinders intraorally. The provisional restoration was tried-in to ensure an absence of binding for complete seating (Figure 15). The provisional restoration was removed and acrylic was placed into the intaglio surfaces (Figure 16), then replaced intraorally and secured with retaining screws inserted into the Conical Temporary Cylinders. The patient was brought into centric occlusion while the acrylic resin set. After setting of the acrylic resin, the two retaining screws were removed and the bridge was tapped out. The voids around the QuickBridge Caps were filled with cold-cure acrylic resin and the excess acrylic was removed. The completed provisional restoration was reseated intraorally using bite sticks and retained with screws inserted into the two Conical Temporary Cylinders (Figure 17). The final implant locations can be seen in Figure 18.
CLINICAL OVERVIEWThis clinical case presentation demonstrates the use of CT-guided implant surgery in the edentulous maxilla. The treatment plan provided for the placement of multiple implants using a minimally invasive, flapless surgical protocol, followed by the immediate placement of a prefabricated, laboratory-processed, provisional restoration with QuickBridge Provisional Components. All decision-making occurred before surgery in concert with the surgical, restorative, and laboratory teams. Although the apices of the implants are in close proximity to one another, the planning software and the precision of the Navigator System’s surgical instrumentation allowed for accurate implant position without risk of the implant apices impinging upon one another. The ability to incorporate angulated abutments in the plan allowed for a common path of insertion and the location of screw access openings in their appropriate location. For additional case photographs and to view treatment videos, visit www.biomet3i.com and click on IN THE OPERATORY.
DisclosureDrs. Baumgarten and Meltzer are consultants for BIOMET 3i. ReferencesRosenfeld AL, Mandelaris GA, Tardieu PB. Prosthetically directed implant placement using computer software to ensure precise placement and predictable outcomes. Part 1: diagnostics, imaging, and collaborative accountability. Int J Periodontics Restorative Dent. 2006;26(3):215-221. Rosenfeld AL, Mandelaris GA, Tardieu PB. Prosthetically directed implant placement using computer software to ensure precise placement and predictable prosthetic outcomes. Part 2: rapid-prototype medical modeling and stereolithographic drilling guides requiring bone exposure. Int J Periodontics Restorative Dent. 2006;26(4):347-353. Rosenfeld AL, Mandelaris GA, Tardieu PB. Prosthetically directed implant placement using computer software to ensure precise placement and predictable prosthetic outcomes. Part 3: stereolithographic drilling guides that do not require bone exposure and the immediate delivery of teeth. Int J Periodontics Restorative Dent. 2006;26(5):493-439. Sarment DP, Sukovic P, Clinthorne N. Accuracy of implant placement with a stereolithographic surgical guide. Int J Oral Maxillofac Implants. 2003;18(4): 571-577. Van Assche N, van Steenberghe D, Guerrero ME, et al. Accuracy of implant placement based on pre-surgical planning of three-dimensional cone-beam images: a pilot study. J Clin Periodontol. 2007;34(9):816-821. Loubele M, Guerrero ME, Jacobs R, et al. A comparison of jaw dimensional and quality assessments of bone characteristics with cone-beam CT, spiral tomography, and multi-slice spiral CT. Int J Oral Maxillofac Implants. 2007;22(3):446-454. Loubele M, Van Assche N, Carpentier K, et al. Comparative localized linear accuracy of small-field cone-beam CT and multi-slice CT for alveolar bone measurements. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007. In press. Dental Labs Near MeLooking for local dental labs that specialize in dental implant services? The Dental Lab is a leading implant dental lab in the United States. We deliver all over the nation with our fast and reliable shipping services, making us a dental laboratory near you--no matter where you are. Contact us today to get started on your dental implant case. Keywords:
dental surgical guide, implant surgical guide, surgical guide, surgical guide for dental implant, surgical guide implant, dental labs, dental labs near me, local dental labs, dental laboratory near me, dental lab
0 Comments
Leave a Reply. |